Learn to identify the subtle behavioral signs of pediatric OCD, from rigid alignment loops to silent mental compulsions, and discover when unseen cognitive distress requires specialized clinical intervention.
To identify Obsessive-Compulsive Disorder (OCD) in children and teens, you must look beyond typical childhood habits or superstitious routines and spot the presence of rigid, time-consuming patterns. If a young person exhibits intrusive, anxiety-inducing thoughts (obsessions) paired with repetitive behavioral or mental rituals (compulsions) that take up more than an hour a day, it points to a neurobiological condition rather than a temporary behavioral phase. Recognizing these signs early allows for a data-driven medical intervention that can successfully reset a hyper-reactive nervous system and restore daily functioning.

The Neurobiology of OCD: Beyond Simple Cleanliness
A common misconception is that OCD is simply an intense desire for neatness, symmetry, or hand hygiene. In reality, Obsessive-Compulsive Disorder is a complex neurobiological condition rooted in a communication breakdown between the front part of the brain (the prefrontal cortex) and deeper structural networks (the basal ganglia).
When a young person struggles with OCD, their brain’s internal “error message” system becomes hyperactive. The brain sends out persistent, false alarms of danger or contamination that the child cannot logically dismiss. To quiet this overwhelming, daytime internal noise and find temporary relief from intense anxiety, the child feels an uncontrollable, biological drive to perform repetitive, rigid routines.
Identifying Obsessions vs. Compulsions in Youth
OCD is defined by two primary components that trap a developing nervous system in a continuous loop of distress: obsessions and compulsions. Because children and teenagers have different levels of verbal development and face different lifestyle pressures, these signs manifest uniquely across age groups.
Common Obsessions (The Intrusive Thoughts)
Obsessions are involuntary, intrusive thoughts, images, or urges that trigger profound anxiety, disgust, or doubt. In children and teenagers, these frequently include:
- Contamination Fears: Extreme dread of germs, dirt, bodily fluids, household chemicals, or catching a debilitating illness.
- Fear of Severe Harm: Persistent, catastrophic worries that something terrible will happen to a parent, sibling, or themselves if things are not done "perfectly."
- Symmetry and Exactness: An overwhelming feeling that objects, shoes, books, or writing must be aligned in a specific order, or that actions must be done "evenly" on both sides of the body.
- Taboo or Forbidden Thoughts: In teenagers, this often manifests as intrusive, distressing thoughts regarding morality, religion, or causing accidental harm to others.
- Taboo or Forbidden Thoughts: In teenagers, this often manifests as intrusive, distressing thoughts regarding morality, religion, or causing accidental harm to others.
Common Compulsions (The Repetitive Rituals)
Compulsions are the repetitive, visible behaviors or hidden mental acts a young person performs to neutralize the anxiety caused by an obsession. These include:
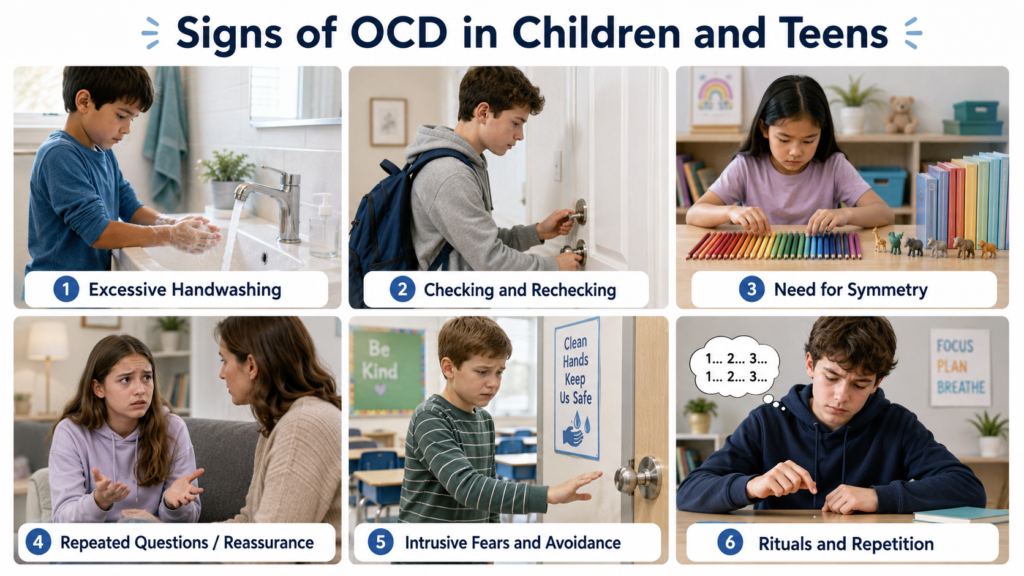
- Excessive Washing and Cleaning: Washing hands until the skin is raw, taking uncharacteristically long showers, or utilizing elaborate, ritualistic wiping routines for school items.
- Checking and Re-checking: Repeatedly checking that doors are locked, light switches are off, appliances are unplugged, or that homework answers are completely correct.
- Repeating and Counting: Feeling forced to step through doorways multiple times, repeating specific words, or counting objects (like floor tiles or ceiling lines) up to a specific number before moving forward.
- Reassurance-Seeking: Constantly asking parents the exact same question (e.g., "Are you sure we won't get sick?") to temporarily quiet internal doubts.
How Childhood OCD Differs from Adolescent OCD
While the underlying neurobiological vulnerabilities remain the same, the presentation of OCD changes significantly as a child transitions into their teenage years.
The Presentation in Young Children
Young children often lack the verbal vocabulary to explain why they feel forced to line up their toys or wash their hands. They operate on a baseline level of emotional dysregulation, showing intense irritability, meltdowns, or unprovoked panic loops when a parent accidentally interrupts a rigid bedtime or morning routine. At this stage, the rituals are highly visible, and parents are frequently dragged into the compulsions (such as being forced to repeat a specific phrase back to the child).

The Presentation in High-Achieving Teenagers
Adolescents face a completely different set of social demands and academic pressures. Because teenagers possess greater self-awareness, they often realize their thoughts and rituals are unusual. To protect their privacy and manage their social standing, they become experts at masking their symptoms.
A teenager’s compulsions often shift inward, becoming entirely mental—such as silently reviewing past conversations, mentally counting, or re-reading text blocks until they feel “just right.” This silent struggle places a massive load on their central nervous system, leading to severe executive burnout, chronic brain fog, and sleep architecture disruption that looks like general depression from the outside.
When to Seek a Private Concierge Evaluation
Many families spend months trying to manage these behaviors through disciplinary measures or standard talk therapy, only to find the rituals becoming more deeply ingrained. When a child’s internal anxiety loop compromises their daily life, a specialized medical intervention is necessary.
A private concierge psychiatrist steps away from high-volume, transactional templates to conduct a deep-dive, unhurried evaluation of your child’s biochemistry, metabolic balance, and nervous system sensitivity. This thorough scientific process ensures that hidden, overactive central nervous system loops are properly identified, which is crucial if the youth is dealing with complex, overlapping conditions like Fibromyalgia and Chronic Pain Treatment or Amplified Musculoskeletal Pain Syndrome (AMPS).
Our Conservative Medication Management Philosophy
A major concern for parents exploring psychiatric support for OCD is the fear of automated, aggressive prescription routines that might blunt their child’s personality or cause permanent side effects.
An elite clinical practice entirely rejects high-volume, default medicating frameworks. We operate strictly under a conservative "Start Low and Go Slow" clinical directive.
Prescriptions are utilized strictly as a targeted, short-term scaffold designed to quiet the baseline neurological “error message” noise, reducing the intensity of intrusive thoughts so that therapeutic coping strategies can take hold. By prioritizing non-habit-forming neuro-modulators at the lowest effective dose, we actively protect early brain development while preserving your child’s core identity, emotional sharpness, and creative drive.
A Faith-Sensitive Framework for Scrupulosity
In values-driven households, a specific type of OCD known as Religious Scrupulosity can cause immense hidden suffering. This manifests as obsessive fears of committing sin, blasphemous thoughts, or an unyielding feeling of moral failure. Children and teens struggling with scrupulosity often internalize their intense anxiety as a spiritual shortfall, carrying an invisible weight of self-blame, thinking their struggles stem from a broken faith or an inadequate prayer life.
Our clinical framework actively deconstructs this narrative by verifying that these intrusive loops are rooted in a measurable, physiological neurobiological condition. We provide a completely private, confidential environment where your Christian convictions are integrated as a primary pillar of healing rather than an afterthought. By treating the human design as an intentional, unified synthesis of neurological pathways and spiritual depth, we ensure your child’s medical plan respects your faith, opening a clear pathway toward sustainable, structural peace.
Frequently Asked Questions
Is it just a childhood phase, or is it actually OCD?
Normal childhood habits, like wanting a specific bedtime story read the same way, provide comfort and are flexible. OCD rituals, however, are rigid, cause profound distress if interrupted, consume more than an hour a day, and actively interfere with school, family life, or social connections.
Can OCD in children and teenagers be treated effectively via telehealth?
Yes. Secure, high-definition telehealth psychiatry is exceptionally effective for youth with OCD. Conducting evaluations virtually allows the physician to assess the child in their natural home environment—where their compulsions and comforts typically play out—while completely removing the stress of travel and public waiting areas.
How should a parent respond when a child demands reassurance during a ritual?
While giving reassurance temporarily calms the child’s anxiety, it actually reinforces the OCD loop by teaching the brain that the danger was real. A psychiatrist will help parents learn gentle, supportive frameworks to help the child sit with the uncertainty, breaking the compulsion step-by-step.
How long does a child or teen need to stay on medication for OCD?
Medication is treated as a supportive, short-term scaffold to stabilize hyper-reactive neural signaling. The duration depends entirely on your child’s biological response and how effectively they master behavioral tools. The ultimate goal is to pair conservative pharmacological support with lifestyle adjustments and stress-reduction techniques to safely guide them back to long-term resilience.
Book a Consultation
It’s easy and free!

Andrew Kuiken
Andrew Kuiken, DMSc, PA-C, is a certified physician assistant and the founder of Christian Psychiatry & Wellness. With over a decade of clinical experience, he is dedicated to restoring quality of life through advanced psychiatric care delivered with compassion and precision.




